Daniel Kolinsky MD, Nicholas M Mohr, MD MS & Brian M Fuller, MD, MSCI
Case Scenario
‘Not again,’ you think to yourself as you listen to the dispatch report. “Call for inter-hospital transport. The patient is a 58 year-old male with a recent diagnosis of pneumonia, in the ED with acute respiratory failure, and is now intubated. Needs transport to the ICU.” This presentation is all too familiar. You remember transporting a similar patient two hours ago. How could you forget? He was hypoxic in the 80’s from his pneumonia.
On arrival to the ED, you get report from the nurses. During sign out you notice that the patient’s ventilator settings are different, specifically the tidal volume is substantially higher than the previous patient’s. You remember that lung-protective ventilation improves outcome in patients with ARDS. You wonder if the same lung-protective strategy should be used in patients at risk for ARDS?
Clinical Question
Does the early use of lung-protective ventilation reduce the incidence of ARDS?
Literature Review
Pre-hospital care of the critically ill and injured patient often requires airway management and subsequent mechanical ventilation. Modern transport ventilators can support critically ill patients across the spectrum of illness severity, and also provide more reliable tidal volume and respiratory rates than manual bag-valve positive pressure ventilation. [1] Furthermore, they also free up the advanced care medic to perform other necessary patient care activities. [2]
Although portable mechanical ventilators have advanced critical care transport capabilities, they are not without risk. Ventilator associated lung injury (VALI) is a general term that refers to how a ventilator can propagate injury in already damaged lungs, or initiate injury in at-risk lungs. [3] Lung-protective ventilation aims to mitigate VALI by reducing the mechanical power applied to the lungs. [4] In patients with established ARDS, lung-protective ventilation with low tidal volume and effective PEEP is standard of care. [5-6] There is also a growing body of evidence from critically ill patients in the ICU and operating room demonstrating that low tidal volume ventilation [6-8 mL/kg predicted ideal body weight (PBW)] is associated with improved outcomes in mechanically ventilated patients without ARDS. [7-12] Although the data are not definitive, the current body of evidence suggests that using lung-protective ventilation strategies can mitigate VALI and prevent progression to ARDS.
Pre-hospital transport and the emergency department (ED) are the common entry points into the hospital for critically ill patients, yet only recently has research been devoted to mechanical ventilation in these arenas. Low tidal volume ventilation initiated in the ED is more likely to be continued in the ICU. [13-14] Additionally, it has been demonstrated that the mechanical ventilation strategy started in the pre-hospital setting is often continued in the ED and in the ICU.15 Together, these studies demonstrate that “ventilator inertia” is real and reinforce the importance of initiating lung protective ventilator strategies from the outset. Unfortunately, compliance with lung protective ventilation strategies in the pre-hospital setting (13%) and ED (range 27.1%-55.7%) leaves much room for improvement. [13-15]
As more studies show that earlier diagnoses with commensurate time-sensitive interventions for the critically ill improves outcomes, pre-hospital personnel will be expected to implement these new standards into practice. [16] Among these interventions, ventilator management is paramount as mechanical ventilation is one of the most common indications for intensive care. [17-18] Providers transporting these patients in the post-intubation period must think about the potential for VALI, as ARDS develops early in the course of critical illness. [12]
Setting the Ventilator
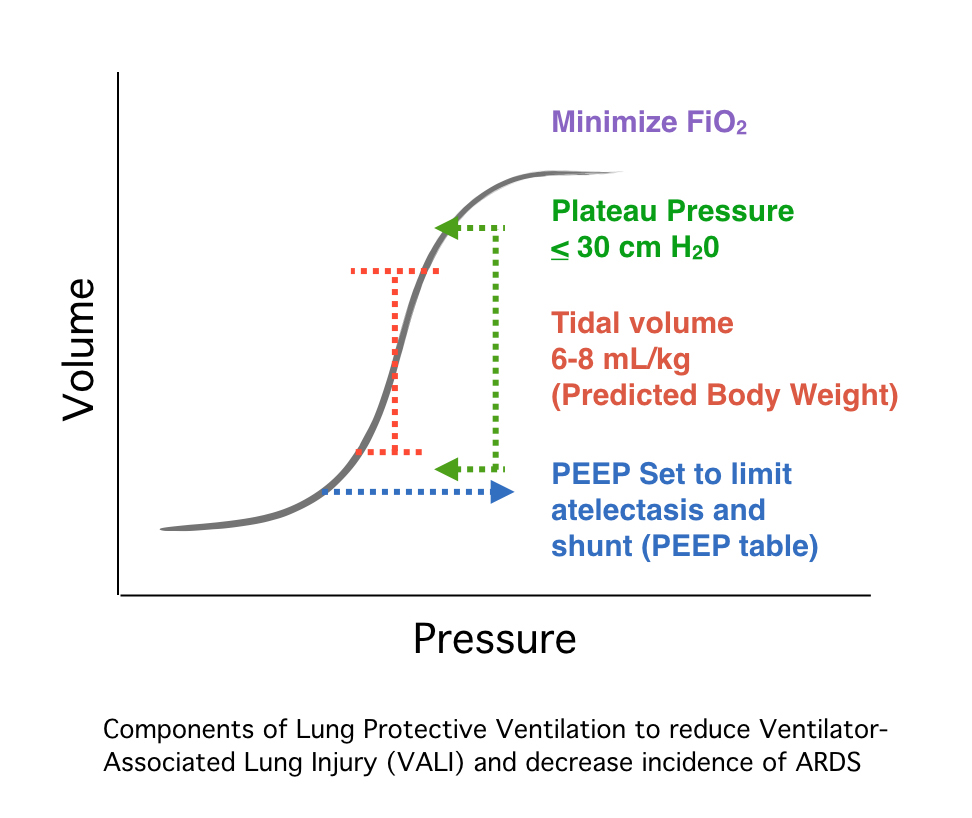
In order to determine the appropriate tidal volume for lung protective ventilation, one needs to know the patient’s gender and height in order to calculate the PBW. PBW can then be derived from a table for low tidal volume ventilation.
Other ventilator parameters to monitor when using lung protective ventilation are positive end-expiratory pressure (PEEP) and the plateau pressure. PEEP can be used to keep diseased alveoli open and limit physiologic shunting thus reducing hypoxemia. Setting the PEEP to 5 cm H2O and titrating PEEP and fraction of inspired oxygen (FiO2) combinations using a PEEP table is a simple way to maintain alveolar recruitment and limit derecruitment injury (i.e. atelectrauma). Targeting oxygen saturations of 88% or greater can limit the dangers of hyperoxia as well.[19] Additionally, maintaining plateau pressures less than 30 cm H2O helps to limit alveolar stretch.
Take Home Points
Acknowledgement that the pre-hospital period is part of the continuum of critical care has led to a focus on implementing best care practices early. In the intubated patient, this includes ventilator management and institution of lung-protective ventilation. Currently, there is a growing body of evidence for using lung-protective ventilation to reduce VALI and to prevent to ARDS. Several large studies testing prophylactic lung protective ventilation are underway. [20-21] Their results will provide further insight into the use of early lung-protective ventilation to improve outcomes.
References
1. Gervais HW, Eberle B, Konietzke D, Hennes HJ, Dick W, “Comparison of blood gases of ventilated patients during transport”. Critical Care Medicine 1987;15:761-763.
2. Weiss, Steven J., et al. “Automatic Transport Ventilator Versus Bag Valve In The EMS Setting: A Prospective, Randomized Trial.” Southern Medical Journal 98.10 (2005): 970-976.
3. Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2013 Nov 28;369(22):2126-36.
4. Gattinoni L, Tonetti T, Cressoni M, Cadringher P, Herrmann P, Moerer O, Protti A, Gotti M, Chiurazzi C, Carlesso E, Chiumello D, Quintel M. Ventilator-related causes of lung injury: the mechanical power. Intensive Care Med. 2016 Oct;42(10):1567-75.
5. The Acute Respiratory Distress Syndrome Network: Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000, 342:1301-1308.
6. Putensen C, Theuerkauf N, Zinserling J, Wrigge H, Pelosi P. Meta-analysis: ventilation strategies and outcomes of the acute respiratory distress syndrome and acute lung injury. Ann Intern Med. 2009;151:566–76.
7. Determann RM, Royakkers A, Wolthuis EK, Vlaar AP, Choi G, Paulus F, et al. Ventilation with lower tidal volumes as compared with conventional tidal volumes for patients without acute lung injury: a preventive randomized controlled trial. Crit Care 2010;14:R1.
8. Mascia L, Pasero D, Slutsky AS, Arguis MJ, Berardino M, Grasso S, Munari M, Boifava S, Cornara G, Della Corte F, Vivaldi N, Malacarne P, Del Gaudio P, Livigni S, Zavala E, Filippini C, Martin EL, Donadio PP, Mastromauro I, Ranieri VM. Effect of a lung protective strategy for organ donors on eligibility and availability of lungs for transplantation: a randomized controlled trial. JAMA. 2010 Dec 15;304(23):2620-7.
9. Futier E, Constantin JM, Paugam-Burtz C, Pascal J, Eurin M, Neuschwander A, et al. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med 2013;369:428–37.
10. Serpa Neto A, Cardoso SO, Manetta JA, et al. Association between use of lung- protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory dis- tress syndrome: a meta-analysis. JAMA. 2012;308(16):1651-1659.
11. Serpa Neto A, Simonis FD, Barbas CS,et al. Association between tidal volume size, duration of ventilation, and sedation needs in patients without acute respi- ratory distress syndrome: an individual patient data meta-analysis. Intensive Care Med. 2014;40(7):950-970.
12. Fuller BM, Mohr NM, Drewry AM, Carpenter CR. Lower tidal volume at initiation of mechanical ventilation may reduce progression to acute respiratory distress syndrome: a systematic review. Crit Care. 2013;17(1):R11.
13. Fuller BM, Mohr NM, Miller CN, Deitchman AR, Levine BJ, Castagno N, Hassebroek EC, Dhedhi A, Scott-Wittenborn N, Grace E, Lehew C, Kollef MH. Mechanical Ventilation and ARDS in the ED: A Multicenter, Observational, Prospective, Cross-sectional Study. Chest. 2015 Aug;148(2):365-74.
14. Fuller BM, Mohr NM, Dettmer M, Kennedy S, Cullison K, Bavolek R, Rathert N, McCammon C. Mechanical ventilation and acute lung injury in emergency department patients with severe sepsis and septic shock: an observational study. Acad Emerg Med. 2013 Jul;20(7):659-69.
15. Stoltze AJ, Wong TS, Harland KK, Ahmed A, Fuller BM, Mohr NM. Prehospital tidal volume influences hospital tidal volume: A cohort study.J Crit Care. 2015 Jun;30(3):495-501.
16. Seymour CW, Rea TD, Kahn JM, Walkey AJ, Yealy DM, Angus DC. Severe sepsis in pre-hospital emergency care: analysis of incidence, care, and outcome. Am J Respir Crit Care Med 2012;186:1264–71.
17. Esteban A, Anzueto A, Frutos F, et al; Mechanical Ventilation International Study Group. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day interna- tional study. JAMA. 2002;287(3):345-355.
18. Needham DM, Bronskill SE, Calinawan JR, Sibbald WJ, Pronovost PJ, Laupacis A. Projected incidence of mechanical ventilation in Ontario to 2026: preparing for the aging baby boomers. Crit Care Med. 2005;33(3):574-579.
19. Girardis M, Busani S, Damiani E, Donati A, Rinaldi L, Marudi A, Morelli A, Antonelli M, Singer M. Effect of Conservative vs Conventional Oxygen Therapy on Mortality Among Patients in an Intensive Care Unit: The Oxygen-ICU Randomized Clinical Trial. JAMA. 2016 Oct 5.
20. Fuller BM, Ferguson I, Mohr NM, Stephens RJ, Briscoe CC, Kolomiets AA, Hotchkiss RS, Kollef MH. Lung-protective ventilation initiated in the emergency department (LOV-ED): a study protocol for a quasi-experimental, before-after trial aimed at reducing pulmonary complications. BMJ Open. 2016 Apr 11;6(4):e010991.
21. Simonis FD, Binnekade JM, Braber A, Gelissen HP, Heidt J, Horn J, Innemee G, de Jonge E, Juffermans NP, Spronk PE, Steuten LM, Tuinman PR, Vriends M, de Vreede G, de Wilde RB, Serpa Neto A, Gama de Abreu M, Pelosi P, Schultz MJ. PReVENT–protective ventilation in patients without ARDS at start of ventilation: study protocol for a randomized controlled trial. Trials. 2015 May 24;16:226.

