by David Ismael Arbona Calderón, MD
Case Scenario:
A 48 y/o unconscious male presented with dizziness and weakness in his office. On arrival of paramedics, patient is diaphoretic and unresponsive, but with pulse and spontaneous respirations. Initial assessment reveals a glucose level of 23 mg/dL. Paramedics find the patients current medication list in the patient’s wallet. Patient is given IV dextrose and regains consciousness. After returning to baseline the patient is refusing transport and further treatment. How do you proceed?
Literature Review:
Diabetes is one of the most common chronic disease, with estimated diagnosis of 23.1 million people in the United States and another 84.1 million adults with prediabetes.[1] As diabetes continues to increase in our population, hypoglycemic events are rising secondary to the use of insulin and oral hypoglycemic agents. Insulin management has been related to the most serious cases of hypoglycemia, either due to strict goals of keeping normal glucose levels or due to confusion between dosing and type of insulin medication. Other diabetes medications like sulfonylureas have been linked to episodes of hypoglycemia and accidental ingestion in the pediatric population. Although hypoglycemia is more common in type 1 diabetes (T1DM), patients with type 2 diabetes (T2DM) experience a similar frequency of these events as they require more aggressive treatment.
The National Electronic Injury Surveillance System-Cooperative Adverse Drug Event Surveillance (NEISS-CADES) has estimated that around 97,648 ED visits occur annually due to insulin-related hypoglycemia and errors related to diabetes management. It has been accounted that around 10% of ED visits are considered under Adverse Drug Events (ADEs) occur annually.[2]
Around 95% of hypoglycemic events occur outside of medical settings, requiring assistance by family members, other caregivers, or emergency medical services (EMS) personnel.[3] Patients with diabetes might not understand when hospital evaluation is needed for proper management of low blood sugars. EMS personnel carry most of the weight of identifying red flags of hypoglycemic episodes that require further workup as some cases can be fatal. There is a continuous debate in the ambulance service as to whether patients suffering from hypoglycemia need to be transported to the hospital after examination and treatment in the field.[4] While some studies have referred that most cases of hypoglycemia can be successfully treated at the scene, conflictive results have been reported in other cases with complications days later.[5]
On 1991, Thompson et al produced one of the earliest studies of treat and release protocols proposed five criteria that should be met before being released form prehospital care without the need for further treatment:
1. History of either T1DM or T2DM
2. Pretreatment blood sugar of less than 4.4 mmol/L or 80mg/dL
3. Post-treatment blood sugar equal or greater to 4.4 mmol/L or 80mg/dL
4. Return to normal mental status within 10 minutes of treatment
5. Absence of complicating factors that require ED evaluation, such as renal dialysis, chest pain, alcohol, dyspnea, of falls.
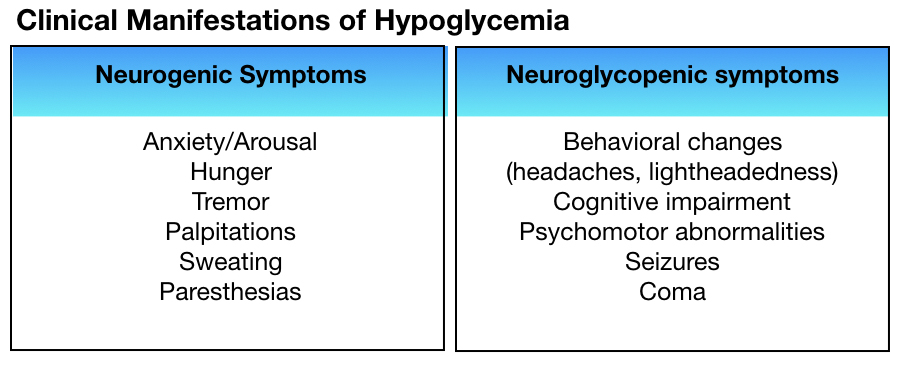
Clinical manifestations of hypoglycemia are nonspecific, and can be divided into neurogenic and neuroglycopenic symptoms.[6]
As reported by NEISS-CADES, patients over 80 years old have a higher risk of being hospitalized due to hypoglycemic events since neuroglycopenic symptoms can mimic other cardiovascular and neurologic conditions.
Other studies regarding younger groups, involving T2DM and over the age of 50 and glycated hemoglobin (HbA1c), suggest that both extreme hyperglycemia and hypoglycemia contribute to poor outcomes when encountering a hypoglycemic event.[7] This can also be applicable for patients with Diabetes Type 1 with extreme values of HbA1c, as recurrent episodes of hypoglycemia and impaired awareness during these episodes are known major risk factors for these events.
Concerns about inappropriate use of sulfonylureas in the elderly and hospitalization rates due to hypoglycemic episodes have been studied.[8] Around one-third of hypoglycemic episodes in the ED were exclusively related to sulfonylurea treatment as they had more prolonged hypoglycemia. Hospital admission of all patients under sulfonylurea treatment with hypoglycemia has been strongly recommended, arguing that regardless resolution of hypoglycemia was done in the ED, observation was needed. Moreover, treatment of hypoglycemia due to sulfonylurea includes octreotide administration. [9]
The National Model EMS Clinical Guidelines (NASEMSO Model) published on 2017, facilitated hypoglycemia protocol.[10] Treatment is focused on level of consciousness and patient disposition will also rely on initial neurological presentation. In a nutshell, a conscious patient with a patent airway can obtain oral glucose, with adults receiving approximately 25 grams of dextrose (at a concentration of 10-50%) and pediatric patients receiving 0.5-1g/kg (at a concentration of 10-25%).
Under NASEMSO Model, an unconscious patient will require Dextrose IV with or without use of Glucagon. A maximum of 25g of 10-50% dextrose IV was determined for adults and for children the 0.5-1g/kg of 10-25% dextrose IV. Patient is in need of transport if hypoglycemic symptoms continue or if patient had a seizure at any point of the episode. Release without transport should only be considered if patient meets all of the following:
- Repeat glucose measurement over than 80mg/dL
- Patient takes insulin or metformin to control diabetes
- Patient returns to normal mental status, with no focal neurologic signs or symptoms after receiving glucose/dextrose
- Patient can promptly obtain and will eat a carbohydrate meal
- Patient or legal guardian refuses transport and EMS providers agree transport not indicated
- A reliable adult will be staying with patient
- No major co-morbid symptoms occur, such as chest pain, shortness of breath, seizures, intoxication
- A clear cause of the hypoglycemia is identified (e.g. skipped meal)
Regardless of National EMS guidelines established for hypoglycemia, there is still variability in EMS protocols throughout the United States. [10-12] Further studies are required to determine the reasons underlying these variations and patient outcome.
Case Scenario Follow-Up:
Patient was given an early lunch at the office, had normal vital signs, and normal EKG. On further questioning patient refers he did not eat breakfast because he was running late for work but did administer his insulin. Patient denied any other symptoms and a coworker is able to stay and watch after the patient. Paramedics used their well person protocol to determine if any abnormalities warranted further intervention. Assessed patient for capacity and oriented the patient about the need for close follow up. Patient indicated he understood all orientations and refused further care.
Take Home:
Any patient with seizures, persistent symptoms of hypoglycemia, and that does not comply with the NASEMSO Model for release without transport criteria should be taken to the emergency department for further evaluation.

References:
[1] Centers for Disease Control and Prevention. National diabetes statistics report: Estimates of diabetes and its burden in the United States, 2017. Atlanta, GA: US Department of Health and Human Services. 2017. https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf [2] Geller AI, Shehab N, Lovegrove MC, et al. National Estimates of Insulin-Related Hypoglycemia and Errors Leading to Emergency Department Visits and Hospitalizations. JAMA Intern Med. 2014;174(5):678–686. doi:10.1001/jamainternmed.2014.136 [3] Lipska, K. J. et al. “Hba1c And Risk Of Severe Hypoglycemia In Type 2 Diabetes: The Diabetes And Aging Study.” Diabetes Care 36.11 (2013): 3535-3542. Web. 9 May 2018. https://doi.org/10.2337/dc13-0610 [4] Roberts, K., and A. Smith. “Outcome of diabetic patients treated in the prehospital arena after a hypoglycemic episode, and an exploration of treat and release protocols: a review of the literature. (Prehospital Medicine).“ Emergency Medicine Journal, May 2003, p. 274+. Health Reference Center Academic. http://link.galegroup.com.ezproxyhost.library.tmc.edu/apps/doc/A102769958/HRCA?u=txshracd2509&sid=HRCA&xid=14527de1 [5] Tohira, H., Fatovich, D., Williams, T. A., Bremner, A., Arendts, G., Rogers, I. R., . . . Finn, J. (2016). Paramedic checklists do not accurately identify post-ictal or hypoglycaemic patients suitable for discharge at the scene. Prehospital and Disaster Medicine, 31(3), 282-293. doi:http://dx.doi.org/10.1017/S1049023X16000248 [6] Hepburn, D. A. et al. “Symptoms Of Acute Insulin-Induced Hypoglycemia In Humans With And Without IDDM: Factor-Analysis Approach.” Diabetes Care 14.11 (1991): 949-957. Web. 9 May 2018. [7] Moheet, Amir, and Elizabeth R. Seaquist. “Hypoglycaemia, Emergency Care And Diabetes Mellitus.” Nature. N.p., 2014. Web. 9 May 2018.doi:10.1038/nrendo.2014.67 [8] Rajendran R, Hodgkinson D, Rayman G. Patients with diabetes requiring emergency department care for hypoglycaemia: characteristics and long-term outcomes determined from multiple data sources. Postgraduate Medical Journal 2015;91:65-71. doi:10.1136/postgradmedj-2014-132926 [9] McLaughlin, S. A., Crandall, C. S., & McKinney, P. E. (2000). Octreotide: an antidote for sulfonylurea-induced hypoglycemia. Annals of emergency medicine, 36(2), 133-138. [10] “National Model EMS Clinical Guidelines”. Nasemso.Org, 2017, http://www.nasemso.org/documents/National-Model-EMS-Clinical-Guidelines-2017-Distribution-Version-05Oct2017.pdf. Accessed 20 May 2018. [10] Paul Rostykus, Jamie Kennel, Kristian Adair, Micah Fillinger, Ryan Palmberg, Amy Quinn, Jonathan Ripley & Mohamud Daya (2016) Variability in the Treatment of Prehospital Hypoglycemia: A Structured Review of EMS Protocols in the United States, Prehospital Emergency Care, 20:4, 524-530, doi: 10.3109/10903127.2015.1128031 [11] Howard H. Moffet, E. Margaret Warton, Lee Siegel, Karl Sporer, Kasia J. Lipska & Andrew J. Karter (2017) Hypoglycemia Patients and Transport by EMS in Alameda County, 2013–15, Prehospital Emergency Care, 21:6, 767-772, doi: 10.1080/10903127.2017.1321707 [12] Khunti, K., Fisher, H., Paul, S., Iqbal, M., Davies, M. J., Siriwardena, A. N. Severe hypoglycemia requiring emergency medical assistance by ambulance services in the East Midlands: A retrospective study. Primary Care Diabetes.2013; (7):159-165.

