Article by Erin Lincoln, MD
Case Scenario:
You are dispatched to a 68-year-old male in cardiac arrest. His family has been performing bystander, and report that he suddenly collapsed just a few minutes ago. CPR is taken over by responding crews, and he is placed on a cardiac monitor/defibrillator. He is found to be in ventricular fibrillation (VF). After several cycles of defibrillation, epinephrine, and amiodarone, the patient remains in cardiac arrest. The medic on scene calls on-line medical control to ask for advice, and specifically asks if calcium can be given, as she has “seen it work before” to get pulses back as a “last ditch effort.”
Background:
Calcium chloride or gluconate was originally utilized in cardiac arrest resuscitation in the 1950’s after a single study was published in 1951 (Kay & Blalock, 1951). However, evidence emerged in the 1980’s demonstrating that calcium chloride had no effect on return of spontaneous circulation (ROSC) rates, and in fact could be detrimental (Landry, Foran, & Koyfman, 2014). Current AHA guidelines do not recommend routine use of calcium in cardiac arrest (Panchal, et al., 2020). Calcium acts as a vasopressor and inotropic agent (Lindqwister, et al., 2020) thus lending itself to a potential drug for cardiac arrest. Calcium is also frequently used in the treatment of hyperkalemia, calcium channel blocker overdose, hypermagnesemia, and hypocalcemia and may be more likely to be used when one of these diagnoses is the suspected cause of cardiac arrest. Additionally, low ionized calcium levels have been correlated with increasing mortality in sepsis and other critical illnesses in adults and children (Bora, Ramazan, Oznur, Emre, & Basar, 2021), (Sanchez, et al., 1989). Thus, calcium may be a drug considered in these and similar etiologies as appropriate due to known association with low calcium and mortality.
However, as calcium is still used for both presumed benefit in special cases, as well as a “last ditch effort” new literature continues to be published addressing the use of calcium in cardiac arrest, including a significant recent RCT.
What does the literature say?
Since the 1980’s, literature has been routinely published regarding the use of calcium in cardiac arrest. Several recent papers have come out, including a double blind, randomized controlled trial of calcium in cardiac arrest, and these papers are nicely summarized in a 2014 Annals of Emergency Medicine article by Landry, Foran, and Koyfman. The take home message: “Irrespective of presenting rhythm, in patients with cardiac arrest, there is no conclusive evidence that administration of calcium during cardiopulmonary resuscitation (CPR) improves survival.” This paper also notes that many of the studies were retrospective, had varied results, and that to truly answer this question, more randomized trials were needed.
Since the publication of this review, several new studies have been published including several randomized controlled trials.
General Adult Medical Cardiac Arrest
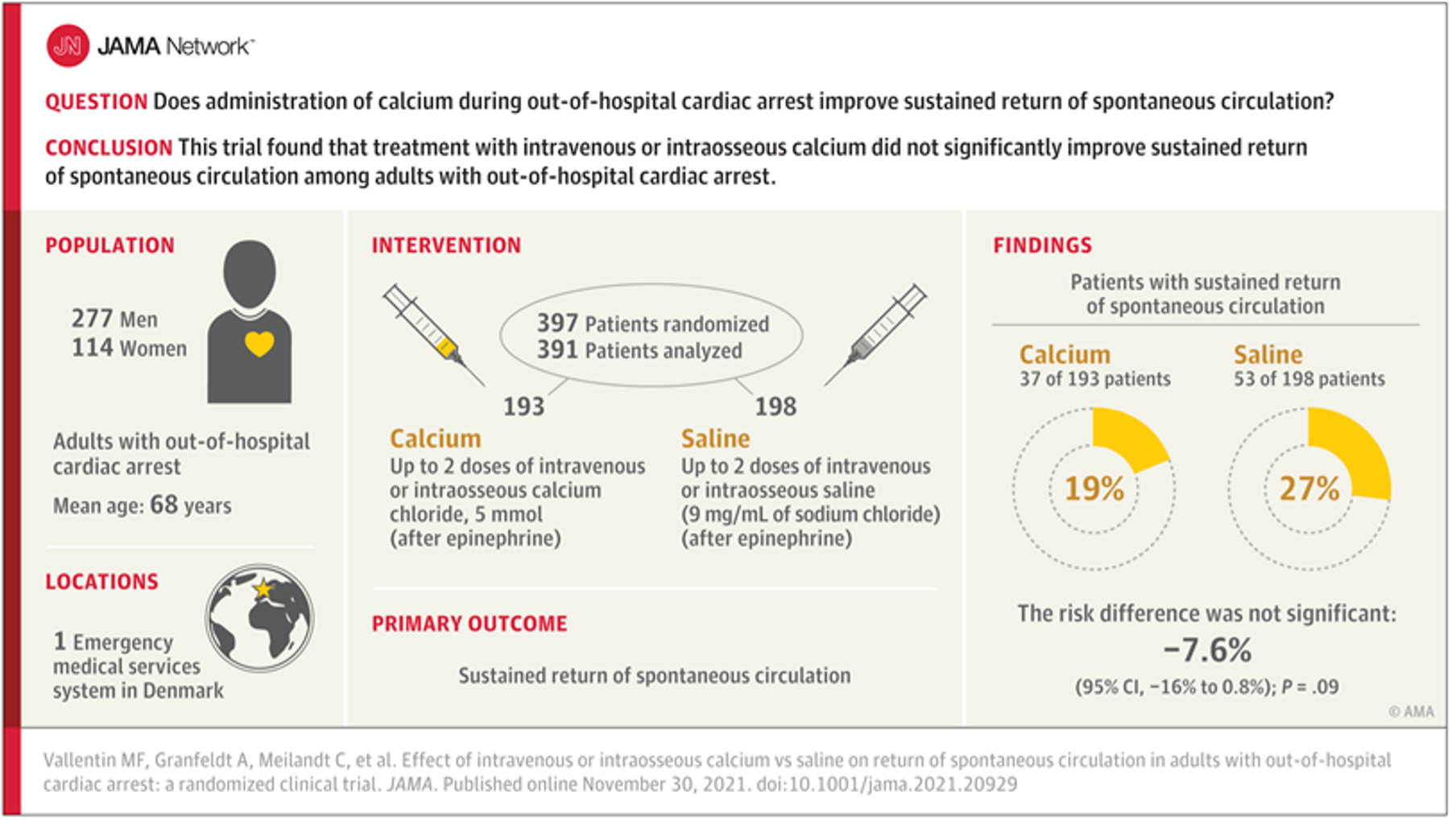
The Calcium for Out-of-hospital Cardiac Arrest (COCA) Trial
This trial was conducted in Denmark and demonstrated through a double blind, randomized, placebo-controlled trial that calcium likely causes harm and was stopped early at a planned interim analysis due to concern for harm in the calcium arm. 397 patients were randomized- 193 received calcium, 198 received saline; of these 37 (19%) of the calcium group achieved ROSC, 53 (27%) of patients in the saline group received ROSC, risk ratio 0.72 [95% CI 0.27-1.18]. This CI does include 1; and further and further analysis of the data showed that the likelihood that calcium has a beneficial effect (e.g. risk ratio >1) was 4% for ROSC, 6% for 30 day survival, and 4% for survival with a favorable neurologic outcome at 30 days (Vallentin, et al., 2021). Visual abstract from this study:
Calcium use during cardiac arrest: A systematic review
This systematic review published in 2022 reviewed prior literature and identified that a meta-analysis was not possible due to only three available RCTs, and only one of those was considered low risk of bias. The overall conclusion was that as less than 1% of cardiac arrest etiologies fall into a group that would potentially benefit from calcium, that routine use should be avoided (Padrao, et. al., 2022).
Association between calcium administration and outcomes during adult cardiopulmonary resuscitation at the emergency department
A small retrospective study from Thailand showed again that there is no benefit to calcium given during Emergency Department resuscitation. This study also reported decreased chances of ROSC in hypocalcemic cardiac arrest patients who received calcium, and potential harm with calcium administration during traumatic arrest. This study did not account for time of administration, so survival bias may have influenced results (Wongtanasarasin, et al., 2022).
Special Cause Cardiac Arrest: Hyperkalemia and Calcium Channel Blocker Overdose
Calcium is regarded as a mainstay treatment for patients with hyperkalemia and EKG changes, and is one of two indications listed in the European Resuscitation Council guidelines on Cardiac Arrest(Lott, et al., 2021), and AHA guidelines also maintain this use (Panchal, et al., 2020). Other AHA/European guideline indications include calcium channel blocker overdose, hypermagnesemia, or hypocalcemia
The effects of calcium and sodium bicarbonate on severe hyperkalaemia during cardiopulmonary resuscitation: A retrospective cohort study of adult in-hospital cardiac arrest
This study out of Taiwan looked at known hyperkalemic cardiac arrests who received both Sodium Bicarbonate (bicarb) and calcium during in-hospital cardiac arrest. The study included 109 hyperkalemic cardiac arrest patients from 2006 through 2012. Of these, 40 (36.7%) patients achieved sustained ROSC, but only four (3.7%) patients survived to hospital discharge. Patients were grouped based on if they received: a) neither calcium nor bicarb; b) bicarb only; c) calcium only; d) calcium AND bicarb. After analysis, bicarb was positively associated with sustained ROSC when serum potassium level was <7.9 mEq/L (odds ratio [OR]: 10.51; 95% confidence interval [CI]: 1.50−112.89; p=0.03); administration of both calcium and bicarb was positively associated with sustained ROSC when serum potassium level was <9.4 mEq/L (OR: 51.11; 95% CI: 3.12−1639.16; p=0.01). This study was limited by small sample size and does NOT look at the effect of calcium alone on known hyperkalemic arrest due to the small available numbers. As no study patients survived with favorable neurologic outcome, no outcome data is available (Wang, et al., 2016).
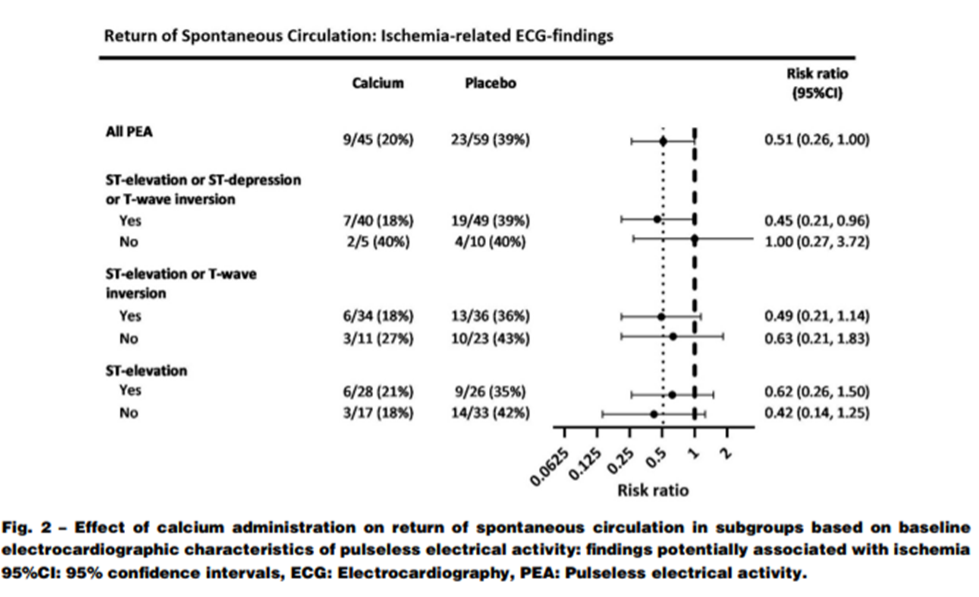
Secondary analysis of COCA Trial
This assessed the effect of calcium in patients with PEA/ECG characteristics that could potentially have been associated with hyperkalemia and ischemia. 104 patients from the trial were found to have PEA as their last known rhythm prior to receiving the trial drug (calcium or placebo). The rhythm obtained by the defibrillator pads was analyzed for signs of hyperkalemia including loss of P waves, wide QRS complexes and large T wave amplitude. Of these patients, 45 received calcium, 59 received placebo; 9 patients (20%) in the calcium group achieved ROSC as compared with 23 patients (39%) in the placebo group (risk ratio 0.51, 95% CI 0.26-1). While this again does not demonstrate statistical significance to imply harm, it certainly suggests that calcium may not be as helpful as previously expected when findings of hyperkalemia are present on EKG. (Vallentin, Povlsen, Granfeldt, Terkelsen, & Andersen, 2022). The forest plot for ROSC summarizes some of this data:
Pediatrics
AHA PALS guidelines recommend against routine administration of IV calcium during pediatric cardiac arrest (Topjian, et al., 2020), but IV Calcium is still used routinely in some cases in the critical care setting, such as congenital heart disease. While literature discussing prehospital administration of calcium in pediatric cardiac arrest is sparse, in-hospital literature suggests not only that calcium doesn’t demonstrate benefit, but also is associated with worse outcomes.
Get With The Guidelines-Resuscitation (GWTG-R) Registry
This study demonstrated worse outcomes in pediatric patients with heart disease who received calcium in cardiac arrest- survival to hospital discharge was 39% in calcium recipients vs. 46% in non-recipients (P=0.02) (Dhillon, Kleinman, Staffa, Teele, & Thiagarajan, 2022).
An editorial responding to this study does suggest that while the above paper is effective in many ways, it fails to fully account for the fact that pediatric patients who receive calcium are most likely sicker at baseline than those who do not receive calcium, and are more likely to have worse outcomes irrespective of calcium administration (Savorgnan & Acosta, 2022).
ICE-RESUScitation Project Secondary Analysis
This in-hospital analysis initially included 1,100 patients and was designed to evaluate a CPR quality improvement bundle vs usual care, researchers also found worse outcomes in patients who received calcium, INCLUDING some subgroups that had previously been hypothesized to have potential to benefit from receiving calcium during CPR including sepsis or renal insufficiency. This study attempted to mitigate bias in pre-arrest characteristics between groups by data weighting and included a PRISM (Pediatric Risk of Mortality) score when available from 2-6 hours prior to the arrest. While this study can still only prove correlation, the weighting of variables reduces bias and further supports the association of the calcium alone and the decline in outcomes (Cashen, et al., 2023).
Take Home Points:
Calcium (chloride or gluconate) is not recommended in routine or unknown etiology cardiac arrest for both adult and pediatric patients, and this is consistent with both the AHA and European resuscitation guidelines. This continues to be supported by new literature. Special causes of cardiac arrest to include hyperkalemia and calcium channel blocker overdose, have limited data regarding efficacy but do still carry the recommendation for calcium administration.
References:
1. Bora, C., Ramazan, K., Oznur, A. N., Emre, A. S., & Basar, C. (2021). Ionized calcium level predicts in-hospital mortality of severe sepsis patients: A retrospective cross-sectional study. Journal of Acute Disease, 10(6), 247-251.
2. Cashen, K., Sutton, R., Reeder, R., Ahmend, T., Bell, M., Berg, R., . . . Meert, K. (2023). Calcium use during paediatric in-hospital cardiac arrest is associated with worse outcomes. In Press.
3. Dhillon, G. S., Kleinman, M. E., Staffa, S., Teele, S., & Thiagarajan, R. (2022, November). Calcium administration during Cardiopulmonary Resuscitation for In Hospital Cardiac Arrest in Children With Heart Disease Is Associated With Worse Survival– A Report From the American Heart Association\’s Get With The Guidelines- Resuscitation (GWTG-R) Re. Pediatric Critical Care Medicine, 23(11), 860-871.
4. Kay, J., & Blalock, A. (1951). The use of calcium chloride in the treatment of cardiac arrest in patients. Surg Gynecol Obstet, 93, 97-102.
5. Landry, A., Foran, M., & Kyofman, A. (2014, August). Does Calcium Administration During Cardiopulmonary Resuscitation Improve Survival for Patients in Cardiac Arrest? Annals of Emergency Medicine, 64(2), 187-189.
6. Lindqwister, A. L., Lampe, J. W., Gould, J. R., Kaufman, C., Moodie, K. L., & Paradis, N. A. (2020, Sep 4). Intravenous calcium as a pressor in a swine model of hypoxic pseudo-pulseless electrical mechanical activity-a preliminary repo. Intensive Care Med Exp, 8(1), 50.
7. Lott, C., Truhlar, A., Alfonzo, A., Barelli, A., Gonzales-Salvado, V., Hinkelbein, J., . . . Soar, J. (2021). European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation, 161, 152-219.
8. Padrao, E., Bustos, B., Mahesh, A., Castro, M., Randhawa, R., Dipollina, C., . . . Besen, B. (2022). Calcium use during cardiac arrest: A systematic review. Resuscitation Plus, 12, 1-9.
9. Panchal, A., Bartos, J., Cabanas, J., Donnino, M., Drennan, I., Hirsch, K., . . . Berg, K. (2020). Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 142, S366-S468.
10. Sanchez, G., Venkataraman, P., Pryor, R., Parker, M., Fry, H., & Blick, K. (1989). Journal of Pediatrics, 114(6), 952.
11. Savorgnan, F. M., & Acosta, S. P. (2022). Calcium Chloride Is Given to Sicker Patients During Cardiopulmonary Resuscitation Events. Pediatric Critical Care Medicine, 23(11), 939-940.
12. Topjian, A., Raymond, T., Atkins, D., CHan, M., Duff, J., Jr., B. J., . . . Schexnayder, S. (2020). Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 142, S469-S523.
13. Vallentin, M., Granfeldt, A., Meilandt, C., Povlsen, A., Sindberg, B., & Andersen, L. (2022). Effect of Calcium vs. placebo on long term outcomes in patients with out of hospital cardiac arrest. Resuscitation, 179, 21-24.
14. Vallentin, M., Granfelt, A., C Meilandt, P. A., Sindberg, B., Holmberg, M., Iversen, B., . . . Mortensen, L. (2021, Dec 14). Effect of Intravenous or Intraosseous Calcium vs. Saline on Return of Spontaneous Circulation in Adults With Out-of-Hospital Cardiac Arrest. JAMA, 326(22), 2268-2276.
15. Vallentin, M., Povlsen, A., Granfeldt, A., Terkelsen, C., & Andersen, L. (2022). Effect of calcium in patients with pulseless electrical activity and electrocardiographic characteristics potentially associated with hyperkalemia and ischemia- sub-study of the Calcium for Out-of-hospital Cardiac Arrest (COCA) trial. Resuscitation, 181, 150-157.
16. Wang, C.-H., Huang, C.-H., Chang, W.-T., Tsai, M.-S., Yu, P.-H., Wu, Y.-W., . . . Chen, W.-J. (2016). The effects of calcium and sodium bicarbonate on severe hyperkalemia during cardiopulmonary resuscitation: A retrospective cohort study of adult in-hospital cardiac arrest. Resuscitation, 98, 105-111.
17. Wongtanasarasin, W., Ungrungseesopon, N., Namsongwong, N., Chotipongkul, P., Visavakul, O., Banping, N., . . . Phinyo, P. (2022). Association between calcium administration and outcomes during adult cardiopulmonary resuscitation at the emergency department. Turkish Journal of Emergency Medicine, 22, 67-74.
Editing by Brian Miller, MD
Website Editing and Layout by EMS MEd Editor James Li, MD


