Background: Hypoxia and hypotension are known to independently increase mortality in patients with severe traumatic brain injury, but their combined effects are less clear. The objective of this study was to evaluate the association between survival with out-of-hospital hypoxia (SpO2 < 90%), hypotension (SBP< 90 mmHg) or both following traumatic brain injury.
Methods: This was a retrospective study utilizing EPIC (Excellence in Prehospital Injury Care) database which links the Arizona State Trauma Registry data with detailed out-of-hospital data for patients with major traumatic brain injury. The EPIC trial (subsequently published) evaluated the effect of implementing out-of-hospital traumatic brain injury guidelines on outcome following major traumatic brain injury. This study analyzed the EPIC pre-intervention cohort, including patients age > 10 years of age and treated between January, 2007 and March 2014.
Blood pressure and oxygen saturation data were evaluated by reviewing every documented measurement for each patient during the out-of-hospital phase of care. A patient was categorized as having hypotension if there was single documented SBP < 90 mmHg and categorized as having hypoxia if there was a single documented SpO2 < 90%. The primary outcome of interest was survival to hospital discharge.
The association between mortality, hypotension and hypoxia was examined by logistic regression with adjustment for potential confounding variables including age, sex, race, ethnicity, payment source, trauma type and head region injury score.
Key Results:
· 13,151 patients met study inclusion criteria. 11,545 (87.8%) had neither hypotension nor hypoxia, 604 (4.6%) had hypotension only, 790 (6.0%) had hypoxia only, and 212 (1.6%) had both hypotension and hypoxia.
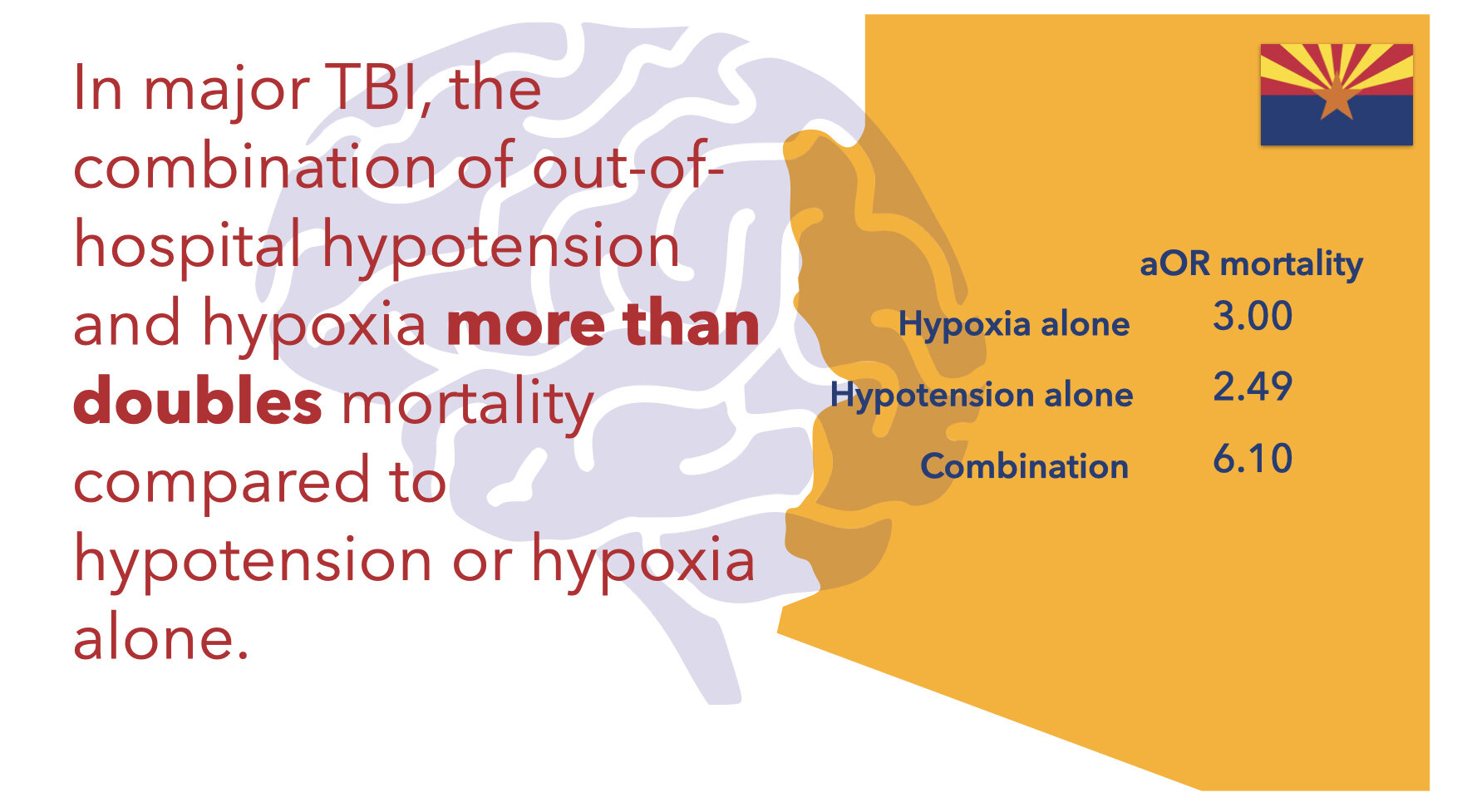
· Hypotension and hypoxia had additive effects on mortality. Adjusted Odds Ratio (aOR) for death in each group was
-
hypotension only: 2.49 (95% CI, 1.87-3.32)
-
hypoxia only: 3.00 (95% CI, 4.20 – 8.86)
-
both hypoxia and hypotension: 6.10 (4.20-8.86)
Conclusions: The combination of out-of-hospital hypotension and hypoxia is associated with more than doubling of the risk of death compared either alone following major traumatic brain injury.
What this Means for EMS: The prehospital phase of care, even though it may be brief, can have dramatic impact on patient survival following traumatic brain injury. This suggests that anticipating and minimizing hypoxia and hypotension as part of a clinical bundle of care may have a dramatic impact on patient mortality, as was confirmed by the EPIC trial results. Incidence of hypoxia and hypotension should be tracked as quality measures for traumatic brain injury.
Article Summary by Maia Dorsett, MD PhD FAEMS, @maiadorsett


