Article: Grunau B, Kime N, Leroux B, et al. Association of Intra-arrest Transport vs Continued On-Scene Resuscitation With Survival to Hospital Discharge Among Patients With Out-of-Hospital Cardiac Arrest. JAMA. 2020;324(11):1058–1067. doi:10.1001/jama.2020.14185
Background
Treatment for a non-traumatic Out-Of-Hospital Cardiac Arrest (OHCA) can occur on scene or during transport. It continues to be the standard in some systems that OHCA patients are transported early, while in other systems patients are treated on scene until return of spontaneous circulation (ROSC) is attained. There is a perception among many in the lay public, hospitals, and even EMS that optimal care is given in the Emergency Department, and all OHCA victims should be transported for best outcomes. However, treatment on scene utilizing similar protocols to the ED until ROSC is felt amongst many to provide a higher quality care than can be attained during transport.
Methods
Data was obtained from the Resuscitation Outcomes Consortium (ROC) registry and collection prospectively from consecutive nontraumatic adult EMS-Treated OHCA. There were 10 sites in North America, data was obtained between 2011 and 2015, and was at the ALS and BLS level. Exclusion criteria included age < 18, a DNR order, cardiac arrest after initiation of transport, or those with missing data. Primary outcome was survival to hospital discharge. Secondary outcome was neurologically-intact survival.
Results
A total of 43,969 consecutive OHCAs were included with 11,625 underwent intra-arrest transport and 32,344 were treated on-scene until ROSC or termination of resuscitation. Survival to hospital discharge was 3.8% for patients who received intra-arrest transport and 12.6% for those who received on-scene resuscitation. Of those transported prior to ROSC, 16% achieved ROSC prior to hospital arrival.
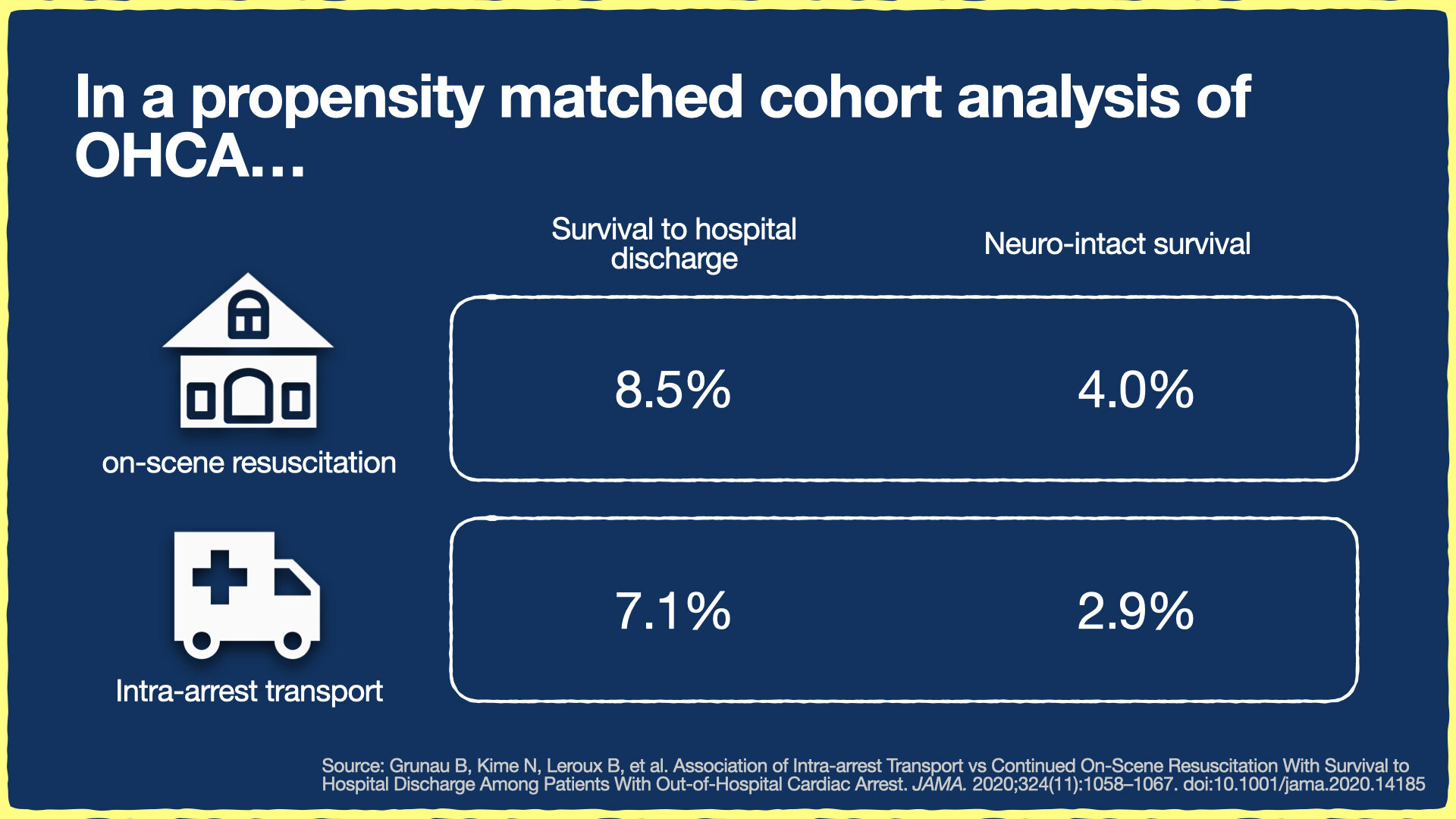
To account for differences between the on-scene resuscitation vs. intra-arrest transport groups, the authors performed a propensity-matched analysis. Survival of intra-arrest transport patients was 4.0%, while survival of transport after ROSC was 8.5%. This result was statistically significant, with an adjusted risk ratio of 0.48 (95% CI, 0.43-0.54). Neurologically-intact survival, defined as a mRS < 3, was also higher in the group with continued on-scene resuscitation: 7.1% for on-scene vs. 2.9% for intra-arrest transport with a statistically-significant adjusted risk ratio of 0.60 (95% CI, 0.47-0.76). This trend held for both shockable and non-shockable rhythms.
What does this mean for EMS?
While not a randomized-controlled trial, this study uses a large prospectively gathered dataset with cohort matching. Therefore the data gathered is likely to represent real-world conditions. In addition this data continues to add to a growing trend of evidence and standard of practice that most patients suffering from cardiac arrest have a higher chance of survival if treated on-scene until ROSC. There are likely subgroups of patients, such as in pregnancy or those who may benefit from eCPR after arrival at a hospital, where transport early or after the 15 minute time mark may lead to some benefit.
Article Summary by Joshua Stilley, MD FAEMS, @JoshuaStilley

