by Aaron Farney, MD
Citation
Background/Rationale
There are two direct laryngoscope blades available to EMS: the curved Macintosh and the straight Miller. Most providers learn to operate both blades, but tend to gravitate towards one based on personal and/or institutional preference. Existing literature suggests the straight blade allows for better visualization, but perhaps intubation is easier with a curved blade. However, there are no existing studies comparing these blades in the prehospital setting. The aim of this study is to compare intubation success with a Macintosh blade versus a Miller blade as performed during pre-hospital endotracheal intubation (ETI) by paramedics.
Methods: This was a retrospective chart review of patients who underwent prehospital ETI from 2007 – 2016 by a single hospital-based suburban EMS service in/near Boca Raton, FL. This system had a 20K EMS volume, double ALS ambulances, 2-tiered system. Intubation attempt was defined as blade passing incisors. Intubation success was defined as confirmation of oxygenation & ventilation following ETI.
Outcomes and results
-
2,299 patients had ETI attempted
-
1,865 attempted with curved blade only (81%)
-
367 attempted with straight blade only (16%)
-
67 attempted using both blades (3% – added to both groups above)
-
Both groups were similar in age, weight, and gender
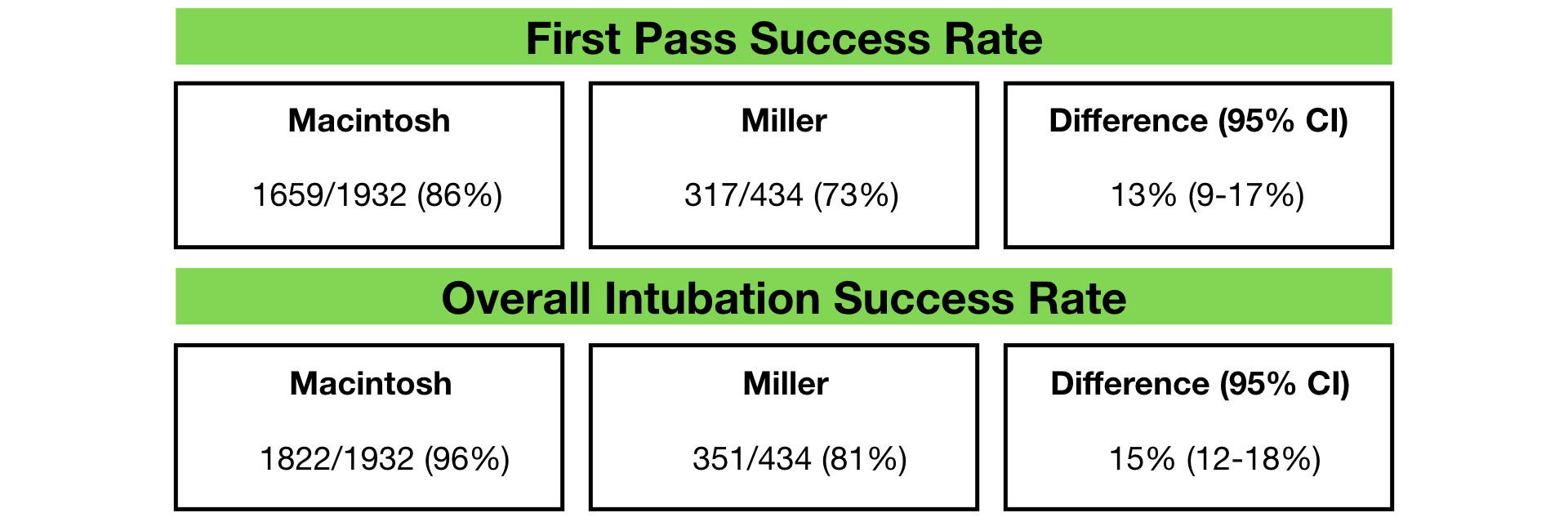
Conclusions: Both first pass success rates and overall intubation success rates for paramedics were significantly higher when Mac blades were used.
Takehome
In this retrospective study, first pass success rates and overall intubation success rates for paramedics were higher when Macintosh blades were used. The difference of 13-15% is expected to be clinically significant. Other process measures such as perintubation hypoxia were not measured. The results of this study demonstrate correlation, not necessarily causation and are subject to confounding variables. For example, the training backgrounds, in particular experience with different blade times, are unknown. However, this is a thought provoking study from the education and training perspective. Should we be stressing training with curved blades or should we focus efforts to improve training with Miller blades or versatility in psychomotor skills?


