by Melissa Kroll, MD and Hawnwan P. Moy, MD
Introduction
The Center for Medicare and Medicaid Services’ (CMS) passage of the Emergency Triage, Treat, and Transport model (ET3) not only recognizes EMS as part of the health care system but is a significant step in developing a mature EMS system. But what does this mean for the EMS medical director? It is unlikely that we will be notoriously ignored like the 1973 EMS System Act of old. But will it help propel the office of the EMS medical director from an often unpaid (or underpaid) position struggling to fulfill the needs of the EMS system to a widely recognized and valued component of the healthcare system? Before we attempt to answer these questions, let’s review what the ET3 model hopes to establish.
What is ET3?
A new model for prehospital care that allows for increased flexibility and efficiency.
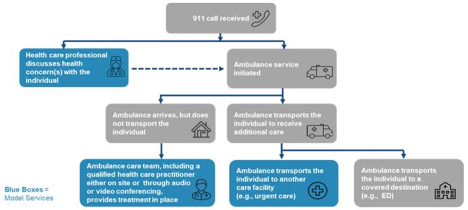
The ET3 Model is a voluntary, five-year payment model aimed at increasing the flexibility and efficiency of prehospital systems. Essentially, with this trial period, CMS has agreed to pay EMS services for the following:
1) transport an individual to an emergency department or other destination covered under the regulations
2) transport to an appropriate destination (such as a primary care doctor’s office or an urgent care clinic)
3) or provide treatment in place with a qualified health care practitioner, either on scene or connected using telehealth.
ET3 hopes this model will encourage cooperative agreements between local EMS systems and surrounding dispatch systems, hospitals, clinics, local governments, etc. This system also allows for increased accountability of systems through monitoring of programs through specific QI/QA metrics.
Feb 14, 2019. Emergency Triage, Treat, and Transport (ET3) Model. https://www.cms.gov/newsroom/fact-sheets/emergency-triage-treat-and-transport-et3-model
What does this mean for the Medical Director?
Not just a “sign here Doc” system.
If we ask any lay person what a good fire or police chief can do for their community, they may not answer with specifics, but they implicitly understand the role of such leadership positions. If you ask them what a good EMS medical director can do for their community, you’re probably going to get a blank stare. Perhaps we have been too complacent in advertising what it is that a good EMS medical director can do for the EMS service and community. Let’s take the opportunity now to highlight what a good medical director can do to ensure the success of ET3 and improve community health.
-
At the heart of it all, a medical director is a physician first. Physicians have duty to ensure that the patient remains at the center of the system -an active medical director ensures that the patient is always number one.
-
With the ET3 expansion of EMS systems there needs to be increased involvement and oversight by medical directors. As experts in the medical direction and having an intimate knowledge of how hospital systems operate as physicians, medical directors are a required leader for connecting the hospital, EMS systems, local governments, and other entities in a collaborative partnership.
-
Many systems will be creating new processes, such as 911 triage, processes for determining optimum patient destination and who can best be treated in the home. New protocols requiring in-depth physician input will need to be developed, trialed, updated, and re-trialed.
-
Constant quality improvement and quality assessment will need to be completed. Continuous quality improvement, quality assessment, and timely feedback by the EMS Medical Director are required to ensure the safe medical care of the patient.
-
Results will need to be published, presented, and discussed allowing for programs to learn from each other. Medical directors will need to be present, both in discussions at a higher level, but also on a ground level where practical application occurs to ensure a smooth maturation of the EMS system for the safety of our patients and still receive valuable data.
-
ET3 allows for treatment to occur in the home in coordination with a qualified healthcare practitioner. Behind every prehospital provider that completes an in-home evaluation, there is the medical director who has provided focused, up to date education, training, and consistent quality assessment.
-
In order to provide treatment in place, there will need to be a conversation with a qualified healthcare practitioner. For many systems, this will be a conversation with their medical director. This medical director will need to be accessible for consultation.
As a subspecialty of medicine, EMS should optimize the opportunity provided by ET3 to move EMS medical direction from “what is” to “what should be”. We would be remiss not to recognize that unfortunately the term “medical director” currently describes a wide range of physician roles – from rubber stamp signatures on paperwork unknown personally to frontline providers to those who are involved in all aspects of patient care provided by an agency. The reason for this spectrum in medical direction is multifactorial. EMS as a medical subspecialty is rather young, although EMS subspecialty fellowship training is working to build a larger base of involved EMS physicians. At the state, agency or regional level, EMS medical directors are often excluded from decision-making. In addition, many medical director positions remain un- or under-funded and full time or majority time EMS physicians are few among us. Reimbursement rates for medical direction (the cost) largely do not acknowledge the value that an involved medical director can bring to the healthcare system. This will be even more evident as we consider treat in place and alternative destinations which will better align patient needs with the current financial incentives of the healthcare market.
The Future
The pilot will end. What needs to happen to make the future successful?
Will a change in reimbursement structure such ET3 be the nidus to move medical direction to where it should be? We think it can. Fundamentally, systems that have relied on rubber stamp physicians will not be able to function in this expanded model. EMS physicians will need to step up to both this challenge and responsibility. Hopefully this new model provides a financial means to support them in doing so.
The ET3 is a 5-year pilot project. Which means it will end. In order to make this a sustainable option in the future, medical directors will not only need to be careful trackers of data, allowing for cost analysis of the impact, but leaders who demonstrate wisdom, integrity, and the expertise required to navigate the unique world of healthcare both in and out of hospitals while keeping an ever-vigilant eye on maintaining patient-focused care. Let’s become the EMS Medical Directors we all strive to be.


