Article Summary by Ian Brodka and Andrew Lee
Article: Grotta, J. C., Yamal, J. M., Parker, S. A., Rajan, S. S., Gonzales, N. R., Jones, W. J., … & Bowry, R. (2021). Prospective, Multicenter, Controlled Trial of Mobile Stroke Units. New England Journal of Medicine, 385(11), 971-981.
Background:
The traditional pre-hospital model for stroke care has been to have EMS clinicians rapidly identify and transport any potential stroke patients from the scene of their stroke to the closest, most appropriate stroke center in order to decrease their time to treatment. At the center of all of this is the tenet: Time is Tissue. So, how do we reduce the time between stroke onset and treatment delivery? One idea is to bring the treatment to the patient through the use of a Mobile Stroke Units (MSUs), which have become available in many urban areas (approximately 20 US and 10 European cities). Given the resource-intensive nature of an MSU, the question remains: do they impact meaningful patient outcomes?
Previous research from Germany in the area of mobile stroke units has demonstrated decreased time from dispatch to thrombolysis [1,2]. One prospective trial from Berlin compared patients treated by the MSU versus those for whom the MSU was not available and found an improvement in functional outcomes at 3 months.[3] With that in mind, the primary objective of this study was to evaluate the impact of mobile stroke unit in multiple US cities on patient disability at three months.
Methods:
This was a prospective, non-blinded, multi-center trial that included all subjects evaluated by EMS/MSU during designated times (e.g. 0800 to 1800, Monday to Saturday) who presented with symptoms consistent with acute stroke, onset within 4.5 hours, and no contraindications to t-PA usage (e.g. evidence of hemorrhage, known intracranial AVM, malignancy, or aneurysm). The enrollment in the trial groups was predetermined by designating each week as an MSU week or an EMS week in an alternating fashion. The subjects were enrolled in the study between August 2014 and August 2020, with varying beginning dates depending on the site.
The primary analysis included only subjects who were deemed eligible for t-PA in a retrospective review by a trained investigator who was blinded to the assigned trial group, whether or not they received t-PA . The primary outcome was the score on the utility-weighted modified Rankin scale at 90 days, which is a patient-centered outcome measure that takes into account patients’ value of functional status. They also assessed various secondary outcomes, which includes changes in the modified Rankin scale of all subjects eligible for t-PA, the percentage of eligible subjects treated with t-PA, and treatment times from stroke onset.
Results:
Of the 1515 subjects enrolled in the study, 1047 of them were included in the final analysis after accounting for t-PA eligibility, subjects lost to follow up, and subjects that withdrew (617 in the MSU group, 430 in the EMS group). A single trial site (Houston) enrolled 77.6% of all the patients; therefore, while it is technically a “multi-center” trial, the overwhelming majority of patients originate from a single center.
Within the treatment groups, 97.1% of the MSU group and 79.5% of the EMS group were ultimately given t-PA as a treatment for their strokes. Across the two groups, controlling factors were nearly identical across age, sex, ethnicity, NIHSS score, and previous strokes.
The key results of the study were the following:
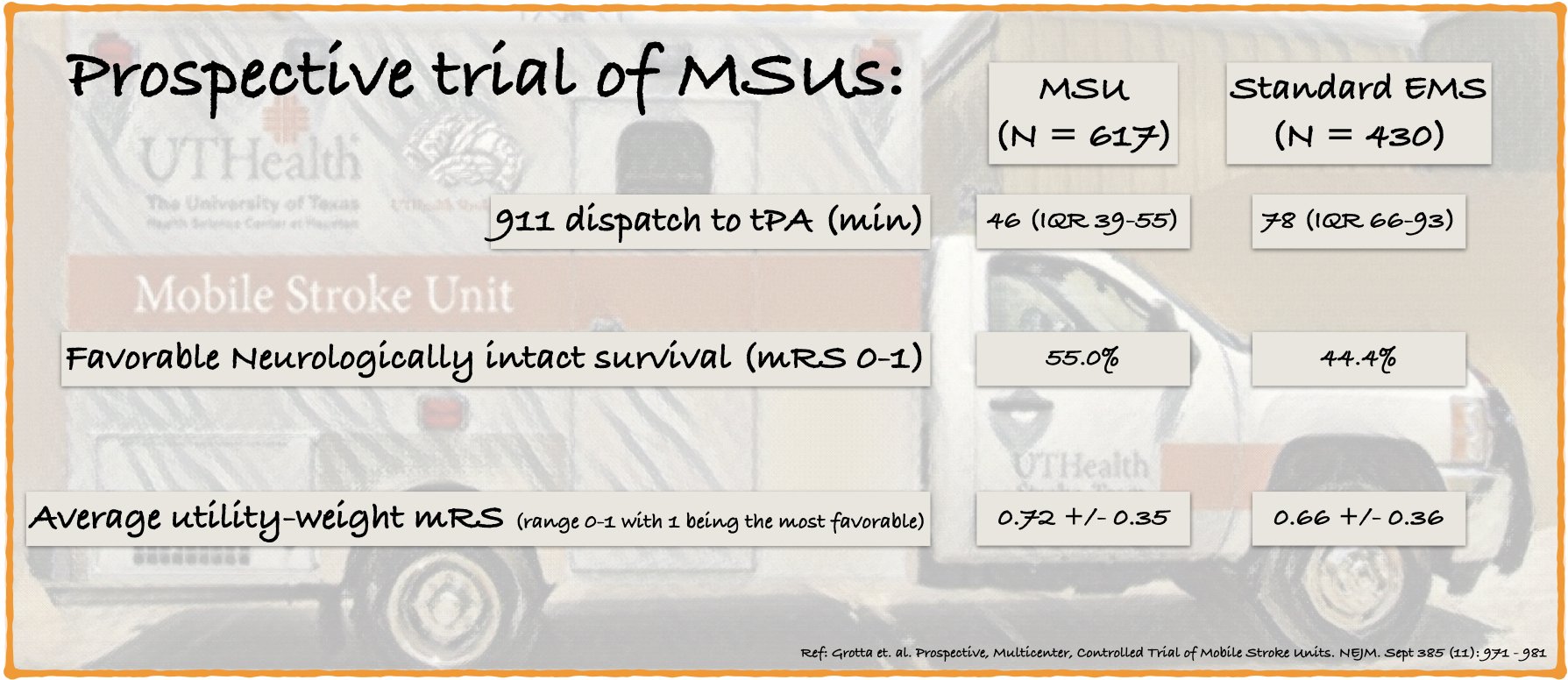
· Median time from last known well to t-PA administration was 72 minutes (IQR 55-105) in the MSU group and 108 minutes (IQR 84-147) in the standard EMS group. Time from 911 alert to t-PA treatment was 46 minutes (IQR 39-55 minutes) for the MSU and 78 minutes (IQR 66-93 minutes) for standard EMS dispatch. Median time from EMS arrival to ED arrival was 55 min (IQR 47-62) for MSU and 27 min (IQR 21-33 min).
· For patients who underwent endovascular therapy, time from EMS alert to EVT start was 141 minutes (IQR 116-171) in the MSU group and 132 minutes (IQR 114-160) in the EMS group. An interesting note as well is that the EMS group has a roughly 10 minute advantage in 911 alert to thrombectomy, but has a 20 minute disadvantage in ED arrival to thrombectomy. The 20 minute delay from arrival to thrombectomy also makes sense in this study, since the EMS group would require the imaging workup to diagnose the stroke in the first place, as opposed to the MSU group diagnosing in the field in the case of availability of CT angiography.
· For the primary outcome of UW-mRS score at 90 days after stroke onset, the MSU group had improvement in functional outcome over the EMS group [MSU 0.72 +/- 0.35 vs. EMS group 0.66 +/- 0.36]. The mean score at discharge was 0.57 +/- 0.37 for the MSU group and 0.51 +/- 0.36 for EMS.
· 55.5% of patients in the MSU group has a mRS of 0 or 1 (good neurologic outcome) compared with 44.4% in the EMS group. Mortality at 90 days was 8.9% in the MSU group and 11.9% in the EMS group.
What this means for EMS:
This study found that Mobile Stroke Units decrease time from 911 notification to t-PA administration and likely improve functional neurologic outcomes for patient suffering from acute ischemic stroke. Implementation of MSUs have been increasing in cities around the country, but their effectiveness must be considered in the context of their environment rather than in isolation. From a system perspective, they are resource intensive and whether they are a cost-effective means to improve community health outcomes remains to be determined.
About the Authors: Ian Brodka and Andrew Lee are third year medical students at the University of Rochester Medical Center. They actively work as EMTs and also run the quarterly EMS Journal club in the Monroe-Livingston Region, during which this article was discussed.
Edited by Maia Dorsett, MD PhD FAEMS, @maiadorsett
References:
1. Walter, S., Kostopoulos, P., Haass, A., Keller, I., Lesmeister, M., Schlechtriemen, T., … & Fassbender, K. (2012). Diagnosis and treatment of patients with stroke in a mobile stroke unit versus in hospital: a randomised controlled trial. The Lancet Neurology, 11(5), 397-404.
2. Ebinger, M., Winter, B., Wendt, M., Weber, J. E., Waldschmidt, C., Rozanski, M., … & STEMO Consortium. (2014). Effect of the use of ambulance-based thrombolysis on time to thrombolysis in acute ischemic stroke: a randomized clinical trial. Jama, 311(16), 1622-1631.
3. Ebinger, M., Siegerink, B., Kunz, A., Wendt, M., Weber, J. E., Schwabauer, E., … & Audebert, H. J. (2021). Association between dispatch of mobile stroke units and functional outcomes among patients with acute ischemic stroke in Berlin. JAMA, 325(5), 454-466.


