Article Summary by: Charles Hwang, MD, FAEMS, FACEP
Background
Extraglottic airway devices (commonly referred to as supraglottic airway [SGA] devices) play an integral role in the prehospital airway algorithm as a primary airway device or as a rescue airway after failed intubation. Recently, two large, randomized controlled trials and a large meta-analysis have demonstrated that, for a variety of medical conditions, SGAs are noninferior to endotracheal intubation with respect to survival-to-discharge, survival with good neurological outcome,[1-3] and first-pass success. As prehospital SGA use will inevitably become more common, hospital clinicians should be familiar with these devices specifically and the role they serve in airway management generally. The indiscriminate rapid and reflexive removal of SGAs without a thoughtful strategy can lead to hypoxemia, aspiration, and/or loss of airway in critically ill patients.
Check out our prior post where our readers discuss their preferred SGAs.
Initial Assessment
There are multiple commercially available extraglottic airway devices. Although they have slightly different features and anatomic positioning, their common attribute is their blind insertion into the oropharynx.
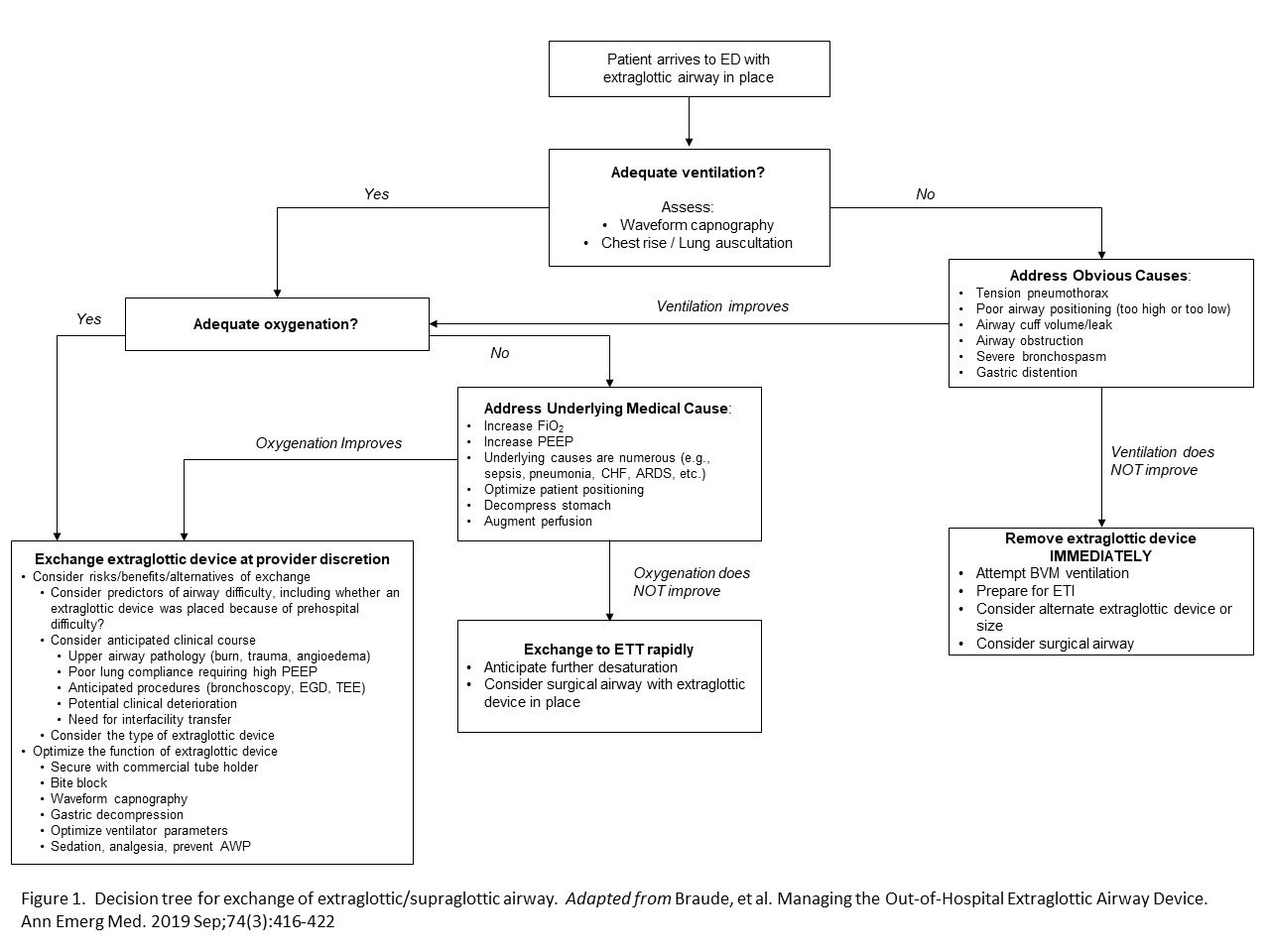
When a patient with an SGA arrives to the emergency department, the ventilation (i.e., waveform capnography, chest rise, lung auscultation) should be assessed, followed by an assessment of oxygenation (i.e., SpO2, PaO2). As is true for endotracheal intubation, it is important to verify waveform capnography to verify tube placement and ventilation adequacy. Intrinsic barriers to ventilation include tube positioning (too high or too low in the oropharynx) and cuff issues. Extrinsic barriers to ventilation are patient factors similar to those experienced while using an endotracheal tube (e.g., pneumothorax, severe bronchospasm, etc.). Similar to endotracheal intubation, impaired oxygenation can be due to atelectasis, underlying medical conditions, and patient positioning, and can be improved by increasing positive end-expiratory pressure (PEEP) and/or fraction of inspired oxygen (FiO2).
Management
The decision to exchange an SGA should depend on two important questions: (1) whether the SGA is providing adequate oxygenation and ventilation and (2) whether the exchange needs to occur electively or urgently. Figure 1 demonstrates the decision tree a clinician should follow when considering these important questions.
Once the decision has been made to exchange the SGA for an endotracheal tube, the SGA can be exchanged using several different methods. The method will depend on patient anatomy, patient stability, anticipated difficulty, and SGA type.
Option 1. Removal of SGA device and standard laryngoscopy
-
Indications: difficult airway not anticipated, favorable physiology, or limited time/equipment.
-
Actions: RSI if patient has intact airway reflexes. Optimize patient positioning and oxygenation. Use SGA to pre-oxygenate. May replace SGA if intubation is unexpectedly difficult.
Option 2. Direct/video laryngoscopy with SGA in place
-
Indications: retroglottic device, which obstructs esophagus and prevents esophageal intubation, is in place (e.g., King Laryngeal Tube, Combitube)
-
Action: Deflate balloon on retroglottic device, sweep device to left with laryngoscope, attempt intubation with endotracheal tube or bougie. May remove retroglottic device if there is an adequate view of airway structures but inadequate access. May reinflate balloon to restore function if unsuccessful intubation.
Option 3. Endoscopic exchange
-
Indications: compatible extraglottic device, adequate time, anticipated difficult intubation.
-
Action: Position device with outlet directly at glottic opening. Pass intubating stylet. Then pass pre-loaded endotracheal tube over stylet (similar to Seldinger technique).
-
An alternative to stylet is the Hennepin double-tube technique which minimizes interruptions in oxygenation and ventilation [4]
Option 4. Blind exchange through extraglottic device
-
Indications: LMA Fastrach, Cookgas airQ, iGel
-
Action: Pass bougie blindly through device into trachea. Must have waveform capnography confirmation. Risks include airway perforation and blind airway technique, which makes this technique less favored.
Option 5. Surgical airway
-
Indications: anticipated difficult airway
-
Action: Surgical cricothyrotomy while oxygenating and ventilating through extraglottic device.
References
1. Benger JR, Kirby K, Black S, Brett SJ, Clout M, Lazaroo MJ, Nolan JP, Reeves BC, Robinson M, Scott LJ, Smartt H, South A, Stokes EA, Taylor J, Thomas M, Voss S, Wordsworth S, Rogers CA. Effect of a Strategy of a Supraglottic Airway Device vs Tracheal Intubation During Out-of-Hospital Cardiac Arrest on Functional Outcome: The AIRWAYS-2 Randomized Clinical Trial. JAMA. 2018 Aug 28;320(8):779-791. doi: 10.1001/jama.2018.11597. PMID: 30167701; PMCID: PMC6142999.
2. Wang HE, Schmicker RH, Daya MR, Stephens SW, Idris AH, Carlson JN, Colella MR, Herren H, Hansen M, Richmond NJ, Puyana JCJ, Aufderheide TP, Gray RE, Gray PC, Verkest M, Owens PC, Brienza AM, Sternig KJ, May SJ, Sopko GR, Weisfeldt ML, Nichol G. Effect of a Strategy of Initial Laryngeal Tube Insertion vs Endotracheal Intubation on 72-Hour Survival in Adults With Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA. 2018 Aug 28;320(8):769-778. doi: 10.1001/jama.2018.7044. PMID: 30167699; PMCID: PMC6583103.
3. White L, Melhuish T, Holyoak R, Ryan T, Kempton H, Vlok R. Advanced airway management in out of hospital cardiac arrest: A systematic review and meta-analysis. Am J Emerg Med. 2018 Dec;36(12):2298-2306. doi: 10.1016/j.ajem.2018.09.045. Epub 2018 Sep 26. PMID: 30293843.
4. Lee DH, Paetow G, Prekker ME, Driver BE. THE HENNEPIN DOUBLE-TUBE TECHNIQUE: A MORE EFFICIENT METHOD OF TRACHEAL INTUBATION THROUGH THE LMA FASTRACH. J Emerg Med. 2022 Jul;63(1):88-92. doi: 10.1016/j.jemermed.2022.04.003. Epub 2022 Aug 5. PMID: 35934655.
Editing by James Li MD, EMS MEd Editor

